In 1982, I attended the golf tournament that’s now called the Honda Classic. I was writing about Tom Watson, who in those days was sometimes referred to in Kansas City, where we both grew up, as “the fourth franchise”. I’d never been to a tour event before, and, in fact, I hadn’t taken up golf yet. It didn’t occur to me that spending a week on a golf course in Florida in March without sunscreen or a hat might be stupid. By the third day, I had burned my nose so badly that what was left of it appeared to have been moulded from strawberry jelly. When I arrived at the press tent the next morning, the guy who checked my credentials said, “Son, you’re in trouble.” The trouble took more than 25 years to emerge, and when it did it was in the form of a wart-like bump on the top of my nose. I assumed at first that the bump was a big, hard pimple. But the usual amateur interventions only seemed to make it worse, so I consulted a dermatologist. He numbed my nose with mini-jabs of Novocain, then used a scalpel to slice off the bump and a fair bit of surrounding tissue. A nurse called later to say that the bump had been basal cell carcinoma, a type of skin cancer. The dermatologist told me that the divot he’d made in my face would eventually fill in with new skin, but that my relationship with cancer wasn’t necessarily over. In both cases, he was right.

Skin cancer is the commonest type of cancer: there are more new cases each year than there are of all other cancers combined. The principal cause is exposure to ultraviolet radiation from the sun, with the usual contributions from genetic bad luck. Basal cell carcinoma is the most widespread and least-frightening variety. It almost never metastasises, and, if the tumour is superficial and small, it can sometimes even be obliterated non-surgically, with repeated applications of a topical cream or with a particular kind of light therapy. Next in severity is squamous cell carcinoma, the treatment for which is trickier but usually also straightforward unless the cancer has spread. The worst kind – and, fortunately, a relatively uncommon one, although its incidence is increasing – is melanoma. If melanoma isn’t caught early, it can metastasise rapidly to distant parts of the body, and once that happens it’s often fatal. Invasive melanoma accounts for a tiny percentage of all skin-cancer cases but for the majority of skin-cancer deaths.
Golfers have always been at greater risk of developing skin cancer than people who never go outside or visit tanning salons, but even among non-golfers the incidence has been rising for years, worldwide. Studies cited by the Skin Cancer Foundation have shown that cases of non-melanoma skin cancer increased by 77 percent from 1994 to 2014, and that there will be 7.7 percent more melanoma cases this year than there were in 2018. (Whales are also affected. They’re exposed to the sun when they surface, and the skin damage they suffer appears similar to the skin damage suffered by humans.) The main cause for the increases is the depletion of the earth’s ozone layer, which is a part of the stratosphere that begins about 15 kilometres up and absorbs ultraviolet radiation that would otherwise broil us. It’s like sunscreen for the entire planet.
The principal enemies of the ozone layer, historically, have been man-made chemicals called chlorofluorocarbons (CFCs), which rise to the stratosphere, decompose in the presence of sunlight, and cause ozone molecules to break apart. For decades, CFCs were used as propellants, refrigerants, foaming agents and solvents in all sorts of common products and machines, including spray deodorants, air-conditioners and fire extinguishers. By the late 1980s, they had become such an obvious threat to human health that almost all the world’s countries agreed to phase out their use.
The ozone layer is far more robust today than it would have been if that agreement hadn’t been reached, but it still provides much less UV protection than it once did. A dozen years ago, I spent a week playing golf in New Zealand during a season when the ozone layer above that part of the world is often especially thin. After a fairly brief exposure, I noticed that the tops of my ears were peeling – a form of UV damage that I hadn’t experienced previously. I’m now on the case.

Every Exposure Counts
An excellent place to study the long-term effects of sunlight on human skin is the PGA Tour Champions. If you look closely at Andy North’s face during one of his appearances as a commentator on ESPN, for example, you’ll notice that his left and right nostrils are different sizes. The reason is that in 1991 – after his wife had pointed out that his nose looked odd – he had surgery to remove a large basal cell carcinoma that extended into his left cheek, followed by plastic surgery to repair the coin-size hole that the excision had created. The USGA persuaded him to write about his experience for Golf Journal, and his article had a big impact on players at all levels. Since that time, he has been an active and effective advocate for skin-cancer prevention and treatment.
North and many other seniors and super-seniors grew up, as I did, in an era when sunburn was viewed as no big deal. In those days, if you applied anything to your skin before going outside, it was almost always in the hope of increasing sun damage, not preventing it. (Sun-darkened skin blocks some UV rays – it’s the body’s attempt at producing its own sunscreen – but the darkening itself is an indicator of damage. “To be clear,” a dermatologist told me, “there is no such thing as a healthy tan.”) My friends and I used to compete, at the swimming pool, to see who could peel the largest intact sheet of skin from his stomach. When I was in college, I fell asleep on a beach in Mexico and burned my back so badly that I had to lean all the way forward in the passenger seat of a friend’s Volkswagen Beetle during our 20-plus-hour drive back to school. The peeling skin hardened into curls the size, shape and approximate colour of Fritos: my back looked as though a woodcarver had worked it over with a chisel. A professor of mine removed the curls by (agonisingly) rubbing me down with cold cream – a service that college professors no longer provide to students, I believe.
“To be clear,” a dermatologist told me, “there is no such thing as a healthy tan.”
Sunlight causes cancer by damaging the DNA in skin cells. The body has a remarkable ability to repair itself, but if UV exposures are sufficiently severe or frequent they can overwhelm the body’s defences. There’s no certainty that the sunburn I got in 1982 was the beginning of my problem, but that interval is typical. Young people often think of skin cancer as a malady of the elderly, but, in fact, sun damage begins in early childhood and accumulates. Every exposure counts, regardless of age, and multiple exposures compound the risk.
Alarmingly, skin cancer patients are getting younger. Adam Scott was treated for a basal cell carcinoma in 2011, when he was 31. “I’d been watching a spot on my nose for a little while,” he said in April, in the clubhouse at the TPC Louisiana, where he was playing in the Zurich Classic of New Orleans. “I had it looked at initially over here, and they said it was nothing to be concerned about. But then, three months later, I had it checked again, in Australia.”
 Australia has the highest skin-cancer rate in the world – like New Zealand, we both sit under a sparse section of the ozone layer each spring – and, as a consequence, even Aussies who aren’t dermatologists often become adept at spotting it. A surgeon removed Scott’s tumour and used skin from his cheek to fill the hole he’d made in the side of his nose. Remember that in 1981, when Scott was a year old, Australia adopted a skin-cancer public-education campaign, whose slogan was “Slip! Slop! Slap!” (slip on a shirt, slop on sunscreen, slap on a hat). Scott’s parents missed that message, but Scott is strictly observant with his two children. He said, “You look at their skin, compared to mine, and you’re just, like, Oh, my god, what happens is horrible.”
Australia has the highest skin-cancer rate in the world – like New Zealand, we both sit under a sparse section of the ozone layer each spring – and, as a consequence, even Aussies who aren’t dermatologists often become adept at spotting it. A surgeon removed Scott’s tumour and used skin from his cheek to fill the hole he’d made in the side of his nose. Remember that in 1981, when Scott was a year old, Australia adopted a skin-cancer public-education campaign, whose slogan was “Slip! Slop! Slap!” (slip on a shirt, slop on sunscreen, slap on a hat). Scott’s parents missed that message, but Scott is strictly observant with his two children. He said, “You look at their skin, compared to mine, and you’re just, like, Oh, my god, what happens is horrible.”
The University of Texas MD Anderson Cancer Center, in Houston, has a marketing relationship with the PGA Tour (and also with a baseball park in Florida and with Houston’s soccer team, the Dynamo). Dermatologists from MD Anderson and its partners provide skin-cancer screenings for players, caddies, fans and members of the media at some tour events, and they distribute free sunscreen, lip balm and sunglasses. I spoke with Susan Chon, a professor of dermatology at MD Anderson. She had recently screened baseball fans during spring training in Palm Beach and was making follow-up calls to make sure that the ones who needed biopsies had gotten them.
“We did a senior PGA event a couple of years ago, at Valero,” she told me. “Those guys are heavily sun-damaged.” When she and her colleagues visit golf tournaments, they sometimes bring liquid nitrogen, which they use to freeze off precancerous lesions called actinic keratoses. “At Valero, literally every golfer we saw needed freezing,” she said. “The younger guys are much more aware. They’ve seen the older generation of golfers ahead of them, and they don’t want to look like that.”
‘The youngerguys are much more aware. They’ve seen the older generation of golfers ahead of them, and they don’t want to look like that.’
Skin cancer is seldom once and for all; people who’ve had it are likely to have it again, and the standard medical advice to anyone who has been treated for any of its varieties is to remain permanently on high alert. In the 28 years since his original surgery, North has had numerous lesions removed from other parts of his body, including his back and his scalp. Last year, I noticed a new bump on my nose, in the crease on the left side. I picked at it for a while, then made an appointment. It turned out to be another basal cell carcinoma, and this time the prescribed treatment was Mohs surgery, a tumour-removal technique that was developed by Frederic E. Mohs beginning when he was a medical student in the 1930s.
My surgeon was Kimberly Eickhorst, who is the Mohs specialist in a dermatological practice in my part of Connecticut. The most appealing feature of Mohs surgery – and the reason it’s still performed, after more than 80 years – is that it has a nearly perfect success record with basal cell carcinoma while keeping tissue-removal to a minimum. “Mohs is skin-sparing,” Eickhorst told me. “With traditional surgery, you remove the basal cell carcinoma and, usually, a five-millimetre margin all the way around it. When you do that, you’re taking healthy skin that you don’t necessarily need to. Mohs is just the opposite. You actually start taking less tissue, but then, if the tumour is still positive in any area, you follow it in that direction.”
Eickhorst kept up a brisk patter as she sliced and snipped a smallish circle of skin from the side of my nose, like cutting a single cookie from a rolled-out sheet of dough. (You can watch her at work on someone else, and hear her description of the technique, by searching YouTube for “Mohs Procedure Derm Westconn” and scrolling down a few videos.) She took the excised tissue to a dedicated Mohs lab down the hall, where she mapped it, dyed it, froze it, sliced it into minutely thin layers, and examined the layers under a microscope – all while I waited. After about 20 minutes, a nurse told me that I had “hit the jackpot”: There were “clear margins” all the way around and under the removed tissue, and that meant no further “stages” would be required. (The average number of stages for most basal cell carcinomas, Eickhorst said, is two.) I had been told to be prepared to stay all day; now I wouldn’t have to.
Eickhorst then put my nose back together, after marking it up with a Sharpie. She was able to shift some skin from an area next to the hole that she had made, and to conceal the scar by running the main incision and the stitches along the crease of my nose. I went home wearing an enormous pressure dressing that covered most of my nose and quite a bit of my left cheek and was instructed to leave it in place for 24 hours. I was also given a list of care instructions, a prescription for a sterile Vaseline-like ointment, a package of gooey yellow gauze, a temporary prohibition against engaging in any exercise vigorous enough to make me sweat, and a supply of enormous Band-Aids. If I’d planned my life better, I’d have gone to the doctor sooner and scheduled my surgery over the winter instead of during the opening weeks of golf season. But all I missed was a couple of tournaments that I’m not wild about anyway.

Scary Cases
Stewart Cink had a basal cell carcinoma removed from the side of his nose in 2018. Two years earlier, Cink’s wife, Lisa, had begun treatment for advanced breast cancer, and some sportswriters (though not Cink) reacted as though their health problems were roughly equivalent: two cancer cases in one couple! But basal cell carcinoma, by comparison with Stage Four breast cancer, is more like a skinned knee than a medical emergency. People don’t die from it, except in the rarest of circumstances, and the treatment doesn’t overturn lives, families and careers.
Melanoma, by contrast, truly is scary. Ellen Flynn – a member of my golf club and an occasional mixed-event partner of mine –has had three melanomas, beginning about 15 years ago. “The first was on the back of my calf, and that wasn’t so terrible,” she told me recently. “Then, four or five years later, I suddenly saw this major mole on my shoulder.” She’d been having regular check-ups with a melanoma specialist, but she couldn’t get an appointment right away. “I didn’t want to be neurotic, but the mole had come from out of nowhere,” she continued. “So I pursued it, and as soon as the doctor saw it I could tell that it wasn’t a good thing.”
The surgeon to whom Flynn’s specialist sent her shocked her by telling her that he couldn’t guarantee that, after the operation, she’d still have the use of her right arm. (“I’m, like, seriously?”) The visible part of a melanoma can be a minor element of a large and rapidly expanding cancer network, and surgeons sometimes have to cut out huge amounts of tissue. Flynn’s tumour, fortunately, turned out to be far less extensive than the surgeon had feared: her golf swing survived. Then, a few years ago, she found a third melanoma, on the shin of her other leg. This one – phew again! – was also neither life nor golf-threatening. “Plus a thousand other skin cancers, on my face mostly,” she said. “So without make-up I look like an ice hockey player.”
 Jonathan Leventhal, a dermatologist and assistant professor at the Yale Cancer Center, in New Haven, Connecticut, told me, “A lot of people think that melanomas start from existing moles, but that’s not actually true. Most melanomas start de novo, meaning on an area of skin that was normal.” On a wall in an examination room he showed me a classic melanoma-identification poster, which used an alphabetic mnemonic, plus photos, to demonstrate what to watch out for. The most common type of melanoma, the poster explained, tends to be Asymmetrical, to have an irregular Border, to be varied in Colour (although the tumour can also be colourless or monochromatic), and to be larger than quarter of an inch in Diameter (although it can also be smaller).
Jonathan Leventhal, a dermatologist and assistant professor at the Yale Cancer Center, in New Haven, Connecticut, told me, “A lot of people think that melanomas start from existing moles, but that’s not actually true. Most melanomas start de novo, meaning on an area of skin that was normal.” On a wall in an examination room he showed me a classic melanoma-identification poster, which used an alphabetic mnemonic, plus photos, to demonstrate what to watch out for. The most common type of melanoma, the poster explained, tends to be Asymmetrical, to have an irregular Border, to be varied in Colour (although the tumour can also be colourless or monochromatic), and to be larger than quarter of an inch in Diameter (although it can also be smaller).
Leventhal said that the poster should also have a fifth letter, E, for Evolution. “By that I mean something that’s changing,” he said. “Changing in size, changing in shape, changing in colour, starting to bleed, starting to itch.”
He then showed me what he described as his most useful diagnostic aid: a hand-held, battery-powered device called a dermatoscope. It consists of a magnifying lens ringed by LEDs and is the current version of a medical instrument that has been around since the 17th century. “It’s particularly helpful at distinguishing a seborrheic keratosis, which is just a benign warty growth – like the one you have right over here, on your cheek – from a melanoma,” he said. He handed the dermatoscope to me, and I used it to examine a mole on the butt of his hand. I also studied what he told me were solar lentigines (commonly called liver spots or sun spots) on the backs of my hands. I have fewer of them on my left hand – my golf-glove hand – than on my right.
Ellen Flynn was in her late 50s when she found her first melanoma. That makes her statistically typical – although the statistics are changing. The incidence of melanoma has risen during the past 85 years, from a lifetime risk of roughly 1 in 1,500 in 1935 for people with white skin to something more like 1 in 40 today. (The darker the skin, the lower the risk of skin cancer, although even for people with very dark skin the risk is not zero, and there are melanoma types that are unrelated to sun exposure and appear at similar frequencies across all racial groups.)
Ellen Flynn was in her late 50s when she found her first melanoma. That makes her statistically typical – although the statistics are changing.
Diagnoses among people much younger than Flynn have also increased. Melanoma is now the most common skin cancer among people 15 to 19, the most common cancer of any kind among people in their 20s, and the leading cause of cancer death among women 25 to 30. I realised recently that I know shockingly many people who have had melanomas, including two people who were in their 20s. One of those is Tyler Fairbairn, another occasional golf partner of mine (and a former playmate of my children), who’s now in his mid-30s. “When I was in graduate school, I noticed that I had a kind of dark, raised thing, like the size of a pencil eraser, on my lower back,” he told me. “The surgeon who operated on it made about a two-inch incision and cut out a bunch all around it.”
Melanoma is now the most common skin cancer among people 15 to 19, the most common cancer of any kind among people in their 20s, and the leading cause of cancer death among women 25 to 30.
Flynn’s and Fairbairn’s melanomas had not penetrated far into their skin, and for such cases the cure rate, through surgery alone, has always been high. The truly dangerous melanomas are the relatively few that have metastasised. (Skip Nottberg, a high-school classmate of Tom Watson’s and an acquaintance of mine, died of one of those in 1997, when he was 47.) Hensin Tsao, who is the clinical director of the Melanoma & Pigmented Lesion Center at Massachusetts General Hospital, told me, “The thicker the tumour, and the bigger the tumour, the more likely it is to reach a blood vessel in the skin, crawl into it, and take off into an internal organ.”
Tsao said that as recently as 10 years ago there was very little that could be done for patients whose melanoma has spread to the brain, the liver, the lungs or other body parts, but that several recently developed drugs have turned out to be extremely effective for many patients – so much so that doctors have begun to speak of cures in cases that once would have been considered hopeless.
Among the many challenges with melanoma is that, although 90 percent of cases are related to solar exposure, some types can appear on parts of the body that have seldom, if ever, been exposed to the sun: between two toes, within the folds of the bellybutton, inside the esophagus, on the anus. In Palm Desert a year-and-a-half ago, I played golf with a retired CEO who was undergoing treatment for a melanoma on the tip of a big toe. He said that the cancer had spread to his lymph nodes, an ominous sign, and that the main reason it hadn’t been diagnosed earlier was that its odd location and unusual appearance had fooled his doctor into thinking it was something else. A number of years ago, a nephew of a friend of a friend of mine was told by his ophthalmologist, during a routine eye exam, that he needed to see an oncologist right away. He did so, and learned that what the ophthalmologist had noticed, inside his eyeball, was an ocular melanoma. Six weeks later, he was dead.
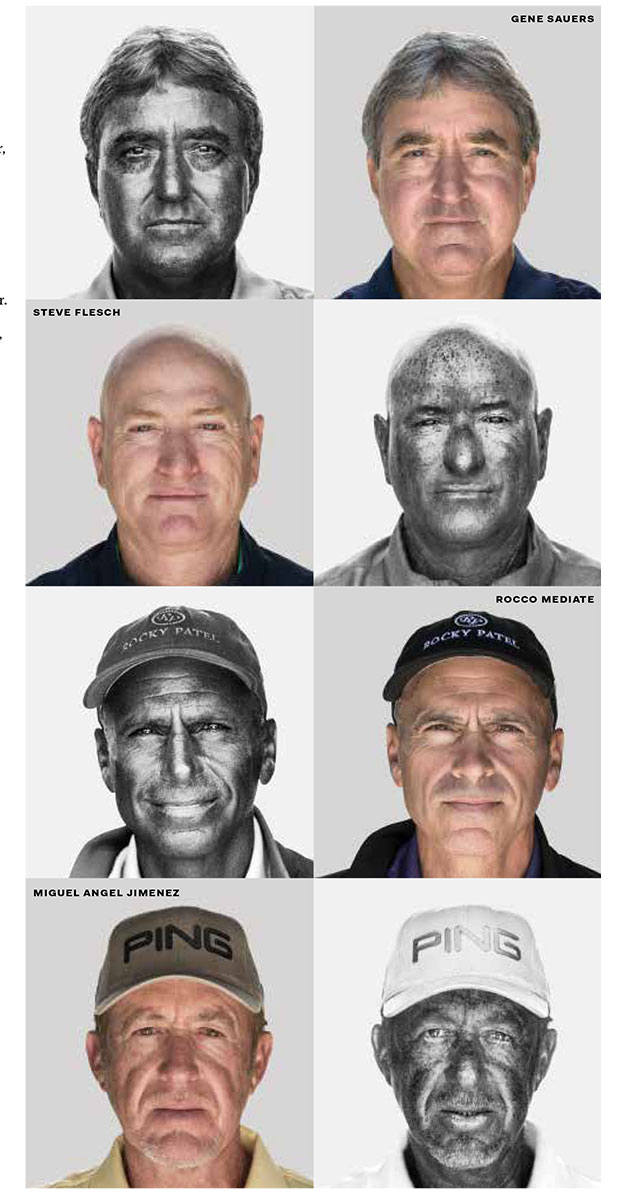 Their careers have been in the sun
Their careers have been in the sun
UV photographs display sun damage in the form of mottled pigmentation because UV light is reduced by melanin. Dark spots indicate sun damage. Golf Digest senior staff photographer Dom Furore photographed PGA Tour Champions players Gene Sauers, Steve Flesch, Rocco Mediate and Miguel Angel Jimenez. Selected comments, as told to Golf Digest senior writer Matthew Rudy:
GENE SAUERS: “In the late ’80s, we would get to Vegas, and I wore a visor at the time. I went home one night and ran a comb through my hair, and it hurt! I said, ‘I need to start wearing a hat and wearing sunscreen.’ We have screenings twice a year out here, and thankfully I’ve never needed to have anything removed. But I’m out here four or five hours a day, and then I go home and hole up inside.”
STEVE FLESCH: “I’m very fair-skinned. I’ve been through my battles of having stuff burned off – pre-cancerous actinic keratosis. I go twice a year and get checked. I’ve had stuff taken off the crown of my head where I got a burn through my hat. It’s moisturiser with sunscreen for me every day on my arms and legs, and more sunscreen on my face. You have to.”
ROCCO MEDIATE: “My skin is different than a lot of the guys out here. You look at some of them, and they’re just toasted.”
MIGUEL ANGEL JIMENEZ “I’m very fair and put lotion on every day.”

KINeSYS sunscreen
A true sport sunscreen, KINeSYS is a golfer’s favourite. The pump spray is easy to apply and the formula is lightweight, non-greasy and fast-absorbing while being sweat resistant. It allows your skin to breathe and sweat as usual, so you don’t have to worry about it clogging your pores and overheating during a round. The company’s fragrance-free sunscreens are available in SPF 30 and SPF 50 and two sizes – a compact travel-size which delivers 170-plus sprays and is perfect for your golf bag or pocket, as well as a 120ml bottle. Available from select retail partners and online at kinesysactive.com.au
Golfersskin sunscreen
Golfersskin’s unique ingredient combination within the formula provides many skin care benefits to the golfer in addition to serious sun protection.
Golfersskin contains Grade Manuka Honey which is scientifically and medically proven to accelerate skin healing, remove harmful bacteria and sterilise infections, stimulate new healthy skin growth, lower incidence of disfiguring scars including acne scars, offer strong anti-inflammatory properties and anti-oxidant support to help fight free radical damage.
Golfersskin’s non-greasy formulation is recommended by the International Melanoma Foundation. E-mail [email protected], phone +64 3 443 4201 or visit golfersskin.co.nz to order.
Key Sun Zinke
Key Sun Zinke is an iconic Australian sun-protection brand that has been closely affiliated with the Australian outdoor lifestyle culture since its inception in 1969. Zinke by Key Sun offers the best possible broad spectrum UVB and UVA protection to help protect against harmful sun rays.
Combined with the latest sunscreen technology and ingredients, Zinke’s formulations provide SPF 30+ and SPF 50+ coverage and four hours water resistance for the best possible protection for your skin under the harsh Australian conditions.
Serious long-lasting, zinc-based sunscreen has proven popular with sportspeople, including golfers, surfers and swimmers. Key Sun Zinke has been protecting Australians since 1969.
Order at keysun.com.au
SParms Sun Protection Shawl UPF 50+
SParms Shawl sleeves are comfortable, cooling and provide excellent quality sun protection. Made from an Italian fabric which is comprised of 90 percent Meryl Microfibre and 10 percent Spandex, this patented material boasts 99.9 percent UV A and B sun protection and is super soft and comfortable.
The connected area to the back allows the product to not slip away, allowing the user intense movements like the golf swing.
With a 50+ UPF rating, you’ll love the cooling and quick-dry capabilities of this product, along with its antibacterial (antimicrobials) properties. Nano Silver technology reduces moisture and odour, keeping you fresh for your entire round.
The shawls are available from small to large and in white, black and steel grey. Order at redbellyactive.com
Tips That Might Save You
I once considered running for US president on a platform that had just three planks. I forget what the first two were, but the third involved requiring people to put on their sunscreen at home, before getting dressed. Many of my golf buddies wait until they’re in our club’s carpark or even on the first tee, and then they not only do a lousy job but also, inevitably, glop up their shirts, pants, gloves and grips. Equally annoying, to me, are parents at the beach who semi-haphazardly smear sunscreen on their squirming, sand-covered kids while the kids are desperately trying to run into the waves. Applying sunscreen at home is easier and more effective. You can do it naked in front of a mirror, you don’t have to work around cuffs, collars, or bikini straps, and when you’re finished you can wash your hands in a sink. Even more important, sunscreen works better and stays on longer if you allow it to soak in.
There are two main categories of sunscreens: physical blockers, which contain opaque particles that reflect ultraviolet radiation, and chemical blockers, which contain substances that convert ultraviolet radiation to heat and disperse it across the surface of the skin. There are unresolved health questions regarding chemical blockers: can they themselves cause cancer? Do their ingredients enter the bloodstream and mimic estrogen or other hormones? Last year, Hawaii banned sunscreens containing two of the most widely used chemical ingredients, octinoxate and oxybenzone, because of damage they do to coral reefs. In February, America’s Food and Drug Administration issued a proposal that will almost certainly result in revisions of its sunscreen regulations. The proposal was prompted mainly by the fact that so little research has been done on the dozen most common active ingredients of chemical sunscreens that the FDA is unable to say that any of them are “generally recognised as safe and effective” (GRASE).
The only active sunscreen ingredients that currently meet the FDA’s GRASE standard are zinc oxide and titanium dioxide, which are the main ingredients of almost all physical blockers. Susan Chon and Kimberly Eickhorst mentioned the same sunscreen brand to me: EltaMD, which is sold mainly by dermatologists but is also available on Amazon and other online outlets. I bought the version that Chon told me she was wearing at the moment we spoke: EltaMD UF Physical, which has a light-brown tint that keeps you from looking like a ghost. “The zinc oxide and titanium dioxide in it are micronised, so it’s not that thick paste you remember from the ’70s or ’80s,” she said. Eickhorst, also, was wearing EltaMD. “It doesn’t cause me to break out, it’s super lightweight, it goes on very translucent, it doesn’t pill, and I can layer it,” she said.

Both dermatologists told me, however, that there are many good brands, of both types, and that the best sunscreen is whichever one you’re the most likely to use. Consumer Reports, which rates sunscreens every year, doesn’t recommend any of the physical blockers; its top choice is Anthelios 60 Melt-In Sunscreen Milk, by La Roche-Posay. Whatever you use, you should keep your sun exposure to a minimum. For golfers, that means, ideally, teeing off either early or late, playing fast, taking advantage of shade when possible, switching from visors and baseball caps to broad-brimmed hats, wearing sunglasses, and covering as much of your skin as you can stand to cover. After speaking with Chon, I bought a pair of solar sleeves, which are thin, stretchy, tight-fitting polyester tubes that you pull up over your bare arms. You’ve probably seen them on TV, most often on LPGA Tour players, who also sometimes carry umbrellas on days when it’s not raining, as sun shields. Putting on solar sleeves is easier (and cheaper) that smearing your arms with sunscreen, and they look less dorky and feel less restrictive than long-sleeved polo shirts. You can even buy ones that make it look as though you’ve been inked from wrist to shoulder. (If I were six inches shorter, I would think about permanently mounting an umbrella on my pushcart. I tried that once, on a blistering day in summer, but couldn’t see where I was going and kept banging my head.)
Ever since my Mohs surgery, I’ve visited my dermatologist’s office twice a year for a full-body skin-cancer inspection – probably a good idea for all avid golfers past a certain age. At my first appointment, the physician’s assistant who examined me told me that she hoped I wouldn’t be “creeped out” by lying on an examination table in front of her in just my underpants, but I told her that I was far more worried about creeping her out. Anyway, we both survived, and I learned that many of the things that bother me about my body have cool-sounding medical names. I also learned that I need to (in Chon’s words) “take ownership” of my skin, by getting to know it as well as I can and then being on the lookout for changes.
I also learned that I need to“take ownership” of my skin, by getting to know it as well as I can and then being on the lookout for changes.
“Your skin is your largest organ,” Eickhorst said. “It’s something that’s with you forever, and you have to take care of it.”
I was negligent until I had a real problem, partly out of laziness and wishful thinking, probably, but also out of ignorance.
Eickhorst continued, “If you ask even medical students what the bad cancers are – or what cancers they have to worry about – the last one on their list is skin cancer, even though it’s by far the most common cancer and the one that’s the most on the rise. We definitely need to pay more attention.”